
Diagnosis: Appendicitis with appendicolith
Bedside ultrasound showed a dilated, tubular structure with no peristalsis in the RLQ that had a hyperechoic 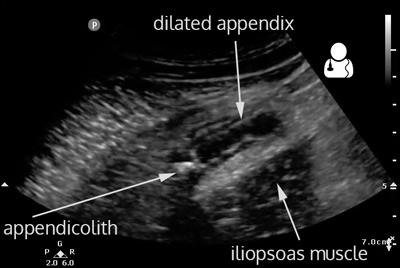 structure in one end, most consistent with an appendicolith. CT showed multiple appendicoliths, with a maximal appendiceal diameter of 1.8 cm. The patient was admitted to the surgery service and in the operating room the surgeons reported seeing a “very inflamed and edematous appendix” that was promptly removed.
structure in one end, most consistent with an appendicolith. CT showed multiple appendicoliths, with a maximal appendiceal diameter of 1.8 cm. The patient was admitted to the surgery service and in the operating room the surgeons reported seeing a “very inflamed and edematous appendix” that was promptly removed.
- The bedside evaluation of the patient with suspected appendicitis should begin at the point of maximal tenderness. If an appendix is not visualized, the RLQ should be examined in a systemic fashion with graded compression.
- The area of evaluation includes a region bordered by the hip laterally and the psoas muscle posteriorly. The iliac artery is another landmark that may assist in the discovery of the appendix as it is often found around it. If the patient has a low enough BMI, you can start with the linear transducer. Otherwise use a curvilinear probe.
- One systematic approach to find the appendix:
- Start low in the right pelvis laterally and identify the iliac crest, probe marker to the right.
- Move the probe medially until you identify the iliopsoas muscle and the iliac vessels.
- Keeping the iliac vessels on the right side of the screen, slowly slide the probe cranially.
- Classically, you will see the appendix snaking over top of the iliopsoas muscle and the iliac vessels.
- Once you identify a possible candidate, follow the structure to ensure that it is a blind pouch, and then follow it laterally and ensure that it goes into the cecum (gas filled structure).
- Last, make sure there is no peristalsis in the suspected appendix. If you see peristalsis, you are looking at small bowel.
- The finding on ultrasound consistent with appendicitis is a dilated, fluid-filled tubular and blind-ended structure that is devoid of peristalsis and has a diameter greater than 6 mm. 1
- Other findings that may point towards the diagnosis of appendicitis are increased vascularity around the suspected appendix, peri-appendiceal fluid and the presence of an appendicolith.1
- Although the specificity of ultrasound in the diagnosis of appendicitis is high, the reported sensitivity has been reported be around 88% in a meta-analysis.2
- The most likely cause of this low sensitivity is the fact that the appendix can be difficult to visualize. This can be due to operator experience or patient factors such as body habitus and presence of interfering bowel gas. 1
- One study that included nearly a thousand pediatric patients from multiple sites reported that the appendix was definitely identified in only 25-56% of examinations.3
- Fortunately, including other information into a diagnostic algorithm increases the negative predictive value of ultrasound.
- Two recent studies combined ultrasound with the white blood cell count. One found that the NPV increased from 41.9% to 95.8% when the white count and ultrasound were used together. 4 Another reported a NPV of 95.59% when ultrasound was combined with the white count when the appendix could not be definitely identified. 5
- Dawson, Mallin. Introduction to Bedside Ultrasound, Volumes 1 and 2. 2013. [inkling]
- Doria AS, Moineddin R, Kellenberger CJ, et al. US or CT for diagnosis of appendicitis in children and adults? A meta-analysis. Radiology 2006;241(1):83-94 [pubmed]
- Mittal MK, Dayan PS, Macias CG, et al. Performance of ultrasound in the diagnosis of appendicitis in children in a multicenter cohort. Acad Emerg Med. 2013;20:(7)697-702. [pubmed]
- Anandalwar SP, Callahan MJ, Bachur RG, et al. Use of White Blood Cell Count and Polymorphonuclear Leukocyte Differential to Improve the Predictive Value of Ultrasound for Suspected Appendicitis in Children. J Am Coll Surg. 2015. [pubmed]
- Cohen B, Bowling J, Midulla P, et al. The non-diagnostic ultrasound in appendicitis: is a non-visualized appendix the same as a negative study? J Pediatr Surg. 2015. [pubmed]
