
Answer: pericardiocentesis
Diagnosis: loculated pericardial effusion with early tamponade
This patient presents with a large, loculated pericardial effusion. There is a large, plethoric IVC suggesting a high CVP. While there is no evidence of RV collapse, the RA does collapse during systole. Left ventricular function is visually normal and there is no evidence of right ventricular dilation or failure. Loculated effusions such as this are more common when scarring has occurred: postsurgical, posttrauma, or purulent pericarditis.1 Large pericardial effusions are not uncommon in patients who have autoimmune disorders and typically accumulate over months.
- When the effusions are chronic the pericardium can accommodate a large volume before causing tamponade physiology, as much as 1 Liter.2
- Conversely, acute pericardial effusions as small at 50-100 mL can cause tamponade because the pericardium has not had a period of time to accommodate the fluid.2
- An IVC with respiratory-phasic changes (>50% collapse with deep breath) suggests a low CVP and rules out tamponade physiology with a 97% sensitivity.3
- The diagnosis of early cardiac tamponade can be made by visualizing right atrial systolic collapse (RASC) on either the subcostal or apical views. Since the RA is the lowest pressure heart chamber, it is the most sensitive finding. Here is an example of RASC:2
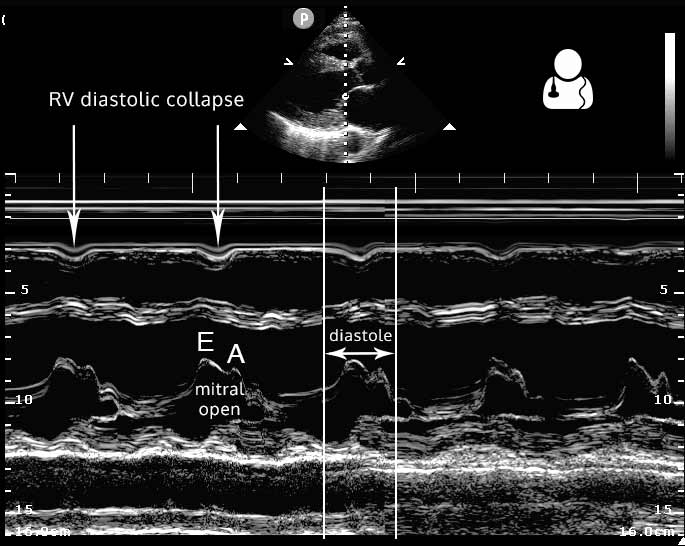
- Right ventricular diastolic collapse (RVDC) is usually easier to identify, but a later finding.2 The echocardiographic appearance of either RVDC or RASC is commonly referred to as the “little man bouncing on a trampoline.” (@jchristianfox first coined this phrase) Notice how in the above clip how the RA and RV alternately collapse, giving a see-saw appearance.
- Slowing the echocardiogram down to look for RASC or RADC frame by frame can be useful and help remove subjectivity from the interpretation. Alternately, using M-Mode across the RV in the parasternal view can show RV wall motion during diastole (same view as EPSS measurement).
- Severe late tamponade physiology results in no appreciable filling of the RV, like in this example of traumatic pericardial clot with tamponade:
- Maisch B, Seferović PM, Ristić AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004;25(7):587-610. [PDF]
- Otto, Catherine M. Textbook of clinical echocardiography. 5th ed. Philadelphia, PA: Elsevier/Saunders, 2013. Print. [Inkling]
- Himelman RB, Kircher B, Rockey DC, Schiller NB. Inferior vena cava plethora with blunted respiratory response: a sensitive echocardiographic sign of cardiac tamponade. J Am Coll Cardiol 1988;12: 1470–7. [pubmed]
